SPECTROstar Nano
Absorbance plate reader with cuvette port


This author profile refers to work created by Dr Andrea Krumm during her tenure at BMG LABTECH - the Microplate Reader Company, where she served as an Applications Specialist contributing scientific content, application notes, and technical expertise. Dr Krumm is no longer employed at BMG LABTECH, but her published materials remain available here for reference and archival purposes. Dr Andrea Krumm is a biotechnology specialist and product manager known for her work in analytical instrumentation and biopharmaceutical analysis. She studied biotechnology and later earned a PhD in cancer biology, focusing on topics such as DNA repair, epigenetics, and tumor biology. After completing her doctorate, she spent several years as an Applications Specialist at BMG LABTECH, where she authored application notes, conducted workshops, and supported scientific customers. In 2020, Dr Krumm joined Tosoh Bioscience GmbH as Product Manager for Analytical Columns.
Our genes define who we are and regulate the myriad of pathways that support life, such as energy provision, movement, and growth. The proteins they encode must acquire the precise structure that enables them to bind specifically with their intended target. A single mutation can prevent a protein from performing its specific role, often with devastating effects.
Many diseases and disorders arise from genetic mutations that interfere with the production of a protein with a key function. The ability to modify or replace defective genes offers the potential to cure a broad spectrum of serious disorders, many of which are otherwise incurable. Indeed, such gene therapy has been a medical goal for several decades.
Recent advances in genomic techniques that enable precise manipulation of gene sequences have provided renewed hope of ground-breaking genetic treatments becoming more widely available to improve, and even save, the lives of patients with genetic diseases. A broad spectrum of gene therapies is being researched, but they typically follow one of three key approaches1. A mutated gene could be replaced by a healthy copy of the gene or inactivated to prevent translation of the malfunctioning protein. If a vital gene is absent or not working, copies of the required gene may be introduced into the body.
Despite its huge therapeutic potential, gene therapy is still an experimental technique and much research remains to be done to ensure the long-term safety of this approach. Consequently, gene therapy is currently limited to diseases for which there is no cure. The indications for which gene therapy is currently being researched include cystic fibrosis, sickle cell anaemia, haemophilia, HIV, muscular dystrophy, and various types of cancer.1
There have been in excess of 2,500 gene therapy clinical studies initiated across a broad range of indications, from infectious diseases to cancer and complex neurodegenerative disorders.2
Cystic fibrosis is caused by a mutation of the gene that produces the cystic fibrosis transmembrane conductance regulator (Cftr). Gene therapies include the introduction of healthy Cftr genes and genome editing to permanently remove mutations in the Cftr gene.3 Similarly, gene therapies have been developed to replace or repair malfunctional dystrophin genes in Duchenne muscular dystrophy.4,5
Anticancer gene therapies that boost the immune response, augment drug effects or interfere with tumour defence mechanisms have proved effective in the treatment of several types of cancer, including melanoma6, prostate cancer7, and lymphoma.8
Research is ongoing at an unprecedented rate, developing more effective and better-targeted ways to deliver gene therapy. Most recently, there has been increasing focus on non-viral gene delivery vehicles, such as nanoparticles9. In addition to disease-modifying treatments, non-viral gene delivery systems have shown great potential as an alternative strategy for tissue repair and regeneration.10
A key factor determining the efficacy of gene therapy is the means by which the gene is introduced. Since genetic material introduced directly into a cell is generally not transcribed, a vector is needed to deliver the therapeutic gene (to restore a missing/malfunctioning protein) or therapeutic RNA (used to modify transcription of an existing gene) into the nucleus.
The vector can be injected in vivo, either intravenously or directly into specific tissue, or mixed with a sample of the patient's cells that are later returned to the patient. The former is generally used to target long-lived post-mitotic cells, whereas the ex vivo approach is needed to infect haematopoietic and other stem cells.
For gene therapy to be successful, it is important that the vector does not elicit an immune response and delivers its genetic cargo to the right cell without interfering with the functioning of other genes. Many of the children who received gene therapy for severe combined immunodeficiency (SCID) subsequently developed T cell leukaemia as a result of insertional mutagenesis.11 An introduced gene must also be effectively transcribed to produce the required protein.
Viruses, having a natural ability to deliver viable genetic material into cells, were an obvious choice of the vector. The therapeutic gene is inserted into the viral DNA and the disease-causing genes are inactivated. When the virus infects a cell, it delivers the inserted gene along with its own but does not cause disease. The viruses most commonly used as gene delivery vectors are adenoviruses, which introduce their DNA into the nucleus of the infected cell, and retroviruses, which integrate their genetic material into the host chromosome.
Limitations of viral vectors drove the search for alternative non-viral gene delivery systems with lower immunogenicity and toxicity, better cell specificity, better modifiability, and higher productivity. These include physical methods, such as biolistics, jet injection, and ultrasound, that enable direct penetration into the cytosol. Such physical systems had the benefit of lower toxicity, but transfection efficacy was low since much of the introduced DNA was degraded before it reached the nucleus.12,13 Chemical transfection was also researched using compounds such as calcium phosphates, lipids, and cationic polymers, but was associated with toxicity.14
Recent successes in tailoring molecular structure and size have increased the efficiency of non-viral transfection and reduced endosomal degradation and toxicity, making them a viable alternative to viral vectors.10
The field of nanotechnology has been advancing rapidly in recent years, providing novel compounds with unique properties to satisfy a wide array of applications. Due to their small size (1 to 100 nm) and high surface-area-to-volume ratio, nanomaterials have great potential as effective non-viral gene delivery systems.15,16 Although transfection efficacy is still lower than with viral vectors, they are less susceptible to reticuloendothelial clearance and exhibit better uptake and internalization than standard non-viral vectors. Furthermore, nanoparticles can be designed to be responsive to an external stimulus or be combined with a specific ligand to enable the time and site of gene delivery to be controlled precisely.17
Various materials (both organic and inorganic) have been investigated for nanoparticle gene delivery, including graphene, gold, lipids, peptides, and other polymers. The genetic material can be either encapsulated within the nanoparticle or conjugated to it via electrostatic binding between the positive charges of the nanoparticle and the negative charges of the DNA.
Nanoparticles of the amine polymer polyethylenimine have been widely studied and are most effective when conjugated to polyethylene glycol (PEG) to reduce non-specific interactions with serum proteins, extend blood circulation time and facilitate accumulation in targeted tissues.15 PEGylated-polyethylenimine-cholesterol (PEG-PEI-cholesterol) gene delivery successfully enhanced expression of the cytokine interleukin 12 in a clinical trial of epithelial ovarian immunotherapy.18 Proteins have also been targeted as gene delivery vectors due to their desirable properties, such as biocompatibility and biodegradability. In addition, their amphilicity allows them to interact with both the solvent and the genetic cargo. Proteins and peptides are commonly combined with inorganic nanomaterials to increase functionalization and incorporate additional desirable properties. A system comprising gelatin and protamine sulphate has achieved efficient gene delivery.19 Similarly, Tat peptide conjugated with silver nanoparticles enabled the delivery of DNA to the nucleus of stem cells with low cytotoxicity.20
The unique properties of the carbon allotrope graphene have made it a particularly attractive gene carrier as it provides high drug loading efficiency, protection from nucleases, and controlled release. Infrared-stimulated gene delivery was achieved with a polyethylene glycol-branched polyethylenimine-reduced graphene oxide (PEG-BPEI-rGO).21
Despite the tremendous potential of nanoparticles as vectors for gene therapy, none has yet been licensed for clinical use. This is largely due to concerns regarding potential health risks that require further investigation, such as body distribution and deposition and direct effects on the central nervous system.
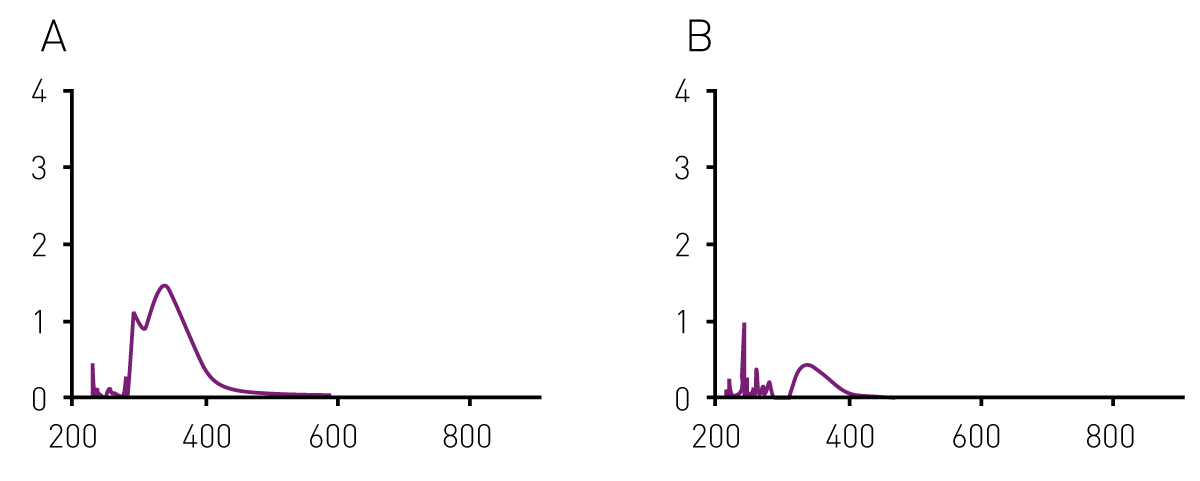
Nanoparticles are characterized in terms of their size, agglomeration state, surface composition, or shape. Some of these characteristics have an impact on their optical properties. Therefore, UV/vis absorbance is used to determine the specific absorbance profile of a nanoparticle suspension and to determine its concentration. Using microplate readers equipped with a UV/vis spectrometer, the analysis can be performed in 96-well microplates. As the absorbance spectrum of a single well is recorded in less than a second, the method is suitable for high throughput analysis of a nanoparticle suspension. The application note “Detection of plant-synthesized nanoparticles and their antibacterial capacity” explains how the SPECTROstar® Nano microplate reader was used to detect nanoparticle formation. The method was further employed by researchers from Texas university: the microplate-based characterization method determined the yield of nanoparticle biosynthesis.22
Another study characterized the cargo of nanoparticles by coupling the cargo (siRNA) to a fluorophore. Measuring the fluorescence intensity of nanoparticles in a CLARIOstar microplate reader reported on the efficiency of non-covalent coupling of siRNA to gold nanoparticles.23
Liposomes closed concentric vesicles of phospholipids, are well established as versatile drug carrier systems due to their biocompatibility, efficacy, and targeting ability.23 They can also transport DNA making them potential non-viral vectors for gene delivery.24,25 Due to the safety advantage and their capacity to accommodate much larger pieces of DNA compared with viral vectors, complexes of cationic phospholipids and a functional gene or DNA, termed genosomes, have been widely studied as gene delivery vectors.
The lipids protect the DNA from degradation during circulation and promote its delivery by bypassing the cell membrane. With improved liposome formulations, such as the use of additives, such as cholesterol to reduce leakage and hemagglutinating virus of Japan to improve transfection, they represent a valuable alternative to viral vectors for gene therapy. PEG is often added to liposomes to improve colloidal stability and reduce aggregation in order to extend their circulation half-life.25 It is now known that such PEGylation of liposomes leads to the spontaneous formation of lipid nanoparticles, which can reduce transfection efficacy. This can be restored by attaching targeting ligands to PEGylated complexes, which has the added benefit of enabling targeted delivery and receptor-mediated uptake.
Research continues to develop genosome formulations with reduced clearance by the reticuloendothelial system and improved transfection rates.25 Genosomes comprising helper lipids of unsaturated dioleoyl chains and phosphatidylethanolamine head groups significantly improved transfection efficiencies of DOPC/DOPE/SS14 lipoplexes.24 Similarly, genosomes prepared using gemini surfactants (two or more head groups and two aliphatic chains linked by a spacer) achieve greater transfection efficiency.27,87 Encapsulation oligonucleotides in stabilized antisense lipid particles have also been shown to be associated with improved cellular uptake.29
Most recently, the advantages of liposomes have been combined with those of nanomaterials with the creation of solid lipid nanoparticles (SLNs) comprising surfactant-stabilized lipids. Studies indicate that SLNs provide effective high-capacity and long-acting non-viral gene delivery with improved transfection efficacy.31,30
Such improvements in liposome structure have increased their potential as gene delivery vectors. However, their use in a clinical setting may only be realised once further research has elucidated the mechanisms of interaction between lipid vectors and gene expression in vivo, and their safety profiles.
Physical methods such as ultrasound can also be used to deliver DNA into a cell by increasing cell membrane permeability. The uptake of DNA by sonoporation has been enhanced using microbubbles (gas-filled spherical voids less than 5 μm in diameter stabilized by a material coating composed of a phospholipid or synthetic polymer). In a high-amplitude, low-frequency ultrasound, the microbubbles rapidly collapse producing liquid jets that can penetrate cells by inducing endocytotic uptake and creating transient pores in the cell membrane.31 Ultrasound itself can be locally targeted to the desired tissue, but the use of microbubbles can facilitate more selective gene delivery through the incorporation of targeting ligands on their surface. The ligands may be antibodies, peptides, or vitamins, depending on the desired target.
Maximum gene expression using microbubble-mediated gene delivery has been shown to be 700-fold greater than ultrasound alone.33 The technique successfully transfected inhibitory RNA into tumour cells preventing angiogenesis and reducing tumour growth34 and achieved gene delivery to mouse myocardium.354 Microbubbles have also been used to deliver genes to the damaged liver to delay or prevent the development of liver fibrosis by regulating the expression of exogenous genes.36 The technique successfully delivered viral DNA vectors to the brain parenchyma, which is otherwise not possible due to the blood-brain barrier, whereby opening up the possibility of gene therapy for genetic disorders of the central nervous system.37
The binding capacity and gene transfection efficiency of microbubbles has been further enhanced by increasing the cationic charge and this has been shown to result in increased therapeutic effect.38 The expression of reporter gene delivered by cationic microbubbles was 20-fold higher in vitro and 3-fold higher in a tumour model compared with neutral microbubbles.39
As with liposomes, microbubbles have been combined with nanotechnology to create nanobubbles.38 These have the added advantage of being able to cross through the blood vessels and achieve greater tumour permeability and retention. Impressive transfection efficacy was reported when ultrasound combined with nanobubbles was used to deliver the tumour necrosis factor to tumour-bearing mice. Treatment resulted in decreased tumour vessel density and inhibition of tumour growth.40
However, it has also been reported that higher microbubble concentrations significantly reduced cell viability without increasing transfection efficiency and prolonged ultrasound exposure decreases the efficiency of gene transfection.32 Furthermore, ultrasound-mediated microbubble gene delivery is a complex, multistep process and further research to understand each of the steps in the process is needed to facilitate optimisation of the technique for clinical applications.40
Viral vectors have been based on many different virus types, but the most commonly used are adenoviruses, adeno-associated viruses (AAV), retroviruses, and lentiviruses. Different viruses enable the delivery of different types of genetic material including both double- and single-stranded DNA or RNA.41
Viral vectors remain the most efficient means of delivering genetic material into host cells. However, due to cases of leukaemia and the death of a young patient after receiving gene therapy in the 1990s, the progress of other viral gene therapies was stalled in favour of less effective but safer non-viral vectors.41
Advances in genetic engineering enabling precision splicing and a greater understanding of gene structure and expression have renewed research efforts into viral gene therapy. A substantial number of gene therapy clinical trials have now been conducted with a range of non-pathogenic, replication-defective viral vectors across many indications.41 The results are promising. For example, intravenous administration of a tumour-selective chimeric adenovirus vector into 17 patients with cancer resulted in tumour-specific delivery with no treatment-related serious adverse events.42 Stem cell-based lentiviral gene therapy resulted in life-long production of Factor VIII, showing the potential to cure haemophilia A.43 Clinical trials are underway for gene therapy lentivirus vectors to inhibit CCR5 and provide protection against HIV.44
There are now approved viral gene therapies that are being successfully used in clinical practice.45 These include a cancer treatment that inserts the CD19 gene into the patient's own T cells ex vivo; when reintroduced the T cells can destroy cancer cells more effectively. Similarly, donor lymphocytes transfected with Herpes simplex virus-1 thymidine kinase and truncated low-affinity nerve growth factor receptors are being used in the treatment of blood cancers. Although not yet approved, a plasmid vector carrying the vascular endothelial growth factor (VEGF) gene, which is directly injected into the target ischaemic tissue, is being developed to cure cystic fibrosis and muscular dystrophy.45
Despite much progress, further research is still required to address concerns regarding current disadvantages, both real and perceived, of viral delivery, such as carcinogenesis, immunogenicity, off-target delivery, random integration of some viral vectors into the host chromosome, and the limitations in the size of the nucleic acid that can be packaged and used for viral gene therapy.45 So, although they offer greater transfection efficiency than non-viral vectors, viral vectors must be proven to be safe before they will again be fully trusted as the most competent gene delivery.
Microplate readers provide the possibility to measure 96 or more samples in one run. This makes them perfectly suited to study different conditions in only one experiment. Research in gene delivery uses this advantage to study the effectiveness of a gene delivery method at the cellular level. For instance, cancer-targeting gene delivery employs cell viability assays such as the colorimetric MTT assay or the fluorescent Resazurin assay to report if cancer cells die following exposure to the cancer-targeted gene delivery system.47 When using fluorescent reporters, microplate readers can be used to measure transfection efficiency with a simple fluorescent readout. A microplate reader further allows a closer look at how gene delivery systems affect cells. As an example, a microplate-based mitochondrial membrane potential (MMP) assay using Rhodamine 12348 can be used to report on mitochondria integrity and cell metabolism in response to gene delivery systems.
Apart from cellular assays, microplate readers determine how much cargo-specific delivery systems carry. This is typically done by labelling the nucleic acid with a fluorophore and acquisition of the fluorescence intensity of the delivering particles.
Dysfunctional genes account for 80% of over 7,000 known diseases and almost 350 million people are affected by genetic diseases globally. Gene therapy, providing the means to correct such disease, thus has huge medical potential. Unlike current treatments for many diseases that merely manage the symptoms or delay progression, gene therapy offers hope of a life-long cure.
The lack of a system to deliver the curative genetic material to the affected cells that is both efficient and safe, in conjunction with difficulties in achieving sustained expression of transgenes has hindered advancements in gene therapy.
Viral vectors provide effective transfection of engineered DNA/RNA but are associated with concerns regarding safety and limitations to the number of nucleotides that than be incorporated into the viral genome. Although there has been tremendous progress in the development of non-viral gene vectors as researchers strive to realise more genetic therapies, poor transfection rates still limit their progress to clinical use.
Recent advances in genomic manipulation and the development of new formulations of non-viral transfection vectors have led to the approval of some gene therapies. There is real hope that further research will lead to the development of a wide range of life-changing gene therapies. Such research is being facilitated by BMG Labtech through the provision of high-quality laboratory equipment. Microplate readers enable efficient evaluation of genetic manipulations, thereby maximising research efforts.
Absorbance plate reader with cuvette port
Powerful and most sensitive HTS plate reader
Most flexible Plate Reader for Assay Development
Upgradeable single and multi-mode microplate reader series
Flexible microplate reader with simplified workflows
Gene reporter assays are sensitive and specific tools to study the regulation of gene expression. Learn about the different options available, their uses, and the benefits of running these types of assays on microplate readers.
ELISAs are a popular tool to detect or measure biological molecules in the life sciences. Find out how microplate readers can be used to advance research using immunoassays.
Antimicrobial resistance is a formidable problem across the world. Find out how microplate readers can help tackle resistant microbes.
Next generation sequencing (NGS) technologies for DNA or RNA have made tremendous progress in recent years. Find out how microplate readers can advance the quality control of nucleic acids to facilitate NGS.
Light scattering offers distinct advantages for scientists interested in immunology. Find out how the NEPHELOstar Plus is used for high-throughput immunological tests.
The LAL assay ensures that sterile pharmaceutical products and medical devices are safe for human use. This test can be run efficiently and in high throughput on a plate reader.