SPECTROstar Nano
Absorbance plate reader with cuvette port


Dr. Carl Peters is the US Applications Science Director with BMG LABTECH. He obtained a PhD in Cell and Molecular Biology from Northwestern University while studying Protein Kinase C signaling. He also has a B.S. in Biology from Hastings College. Prior to BMG LABTECH, he was an adjunct or assistant professor of Biology, Biochemistry and Molecular Biology at several different universities. Carl recently celebrated 13 years with BMG LABTECH. In that time he has become adept at assisting customers with assay development and optimization, including filter selection for unique fluorophores. In addition he has developed skills to help with data analysis in order to streamline customers needs from start to finish. During his time at BMG Carl has been able to expand his knowledge of signal transduction to include high throughput detection of protein-protein interactions. He has also worked with many customers that study neurological disorders that are caused by protein misfolding as they optimize tests to quantify the protein aggregation that results from this misfolding.
There is a long history of the use of antibodies as drugs with the use of monoclonal antibody drugs taking the forefront in these applications in recent history. The first application of antibody-based therapies dates to the work of Emil von Behring who won the first Nobel Prize for Physiology and Medicine in 1901 for his serum therapy that was used as a treatment for diphtheria. The approach involved immunizing animals with toxins, collecting the serum, and using the serum to treat an infectious disease. While quite crude by today's standards, the treatments were still useful and were used fairly routinely until the 1930s.
Of course, the use of monoclonal antibody drugs would not be possible without the advances in basic research which led to hybridoma technology in the mid-1970s. This breakthrough led to a re-emergence of investigation into applications of antibodies as therapies. With the hope that monoclonal antibody drugs would benefit from much higher selectivity of target and hopefully lack some of the negative effects of treating with a heterogeneous solution of serum. In a relatively short amount of time, the first monoclonal antibody drug was approved. Muromonab was approved to help control transplant rejection.
This initial success led to high hopes for monoclonal antibody drugs, but this enthusiasm was tempered by the failure of subsequent treatments derived from mouse hybridomas because of failures in safety and efficacy. It was quickly realized that treatments derived from mice were causing adverse reactions from what became known as human anti-mouse antibodies (HAMA). This understanding has spurred the development of more and more humanized versions of subsequent monoclonal antibody drugs.
Making antibodies more human
The first humanization step was chimeric antibodies which maintained the variable domain from the mouse antibody. This advance led to the first monoclonal antibody drug for the treatment of cancer.
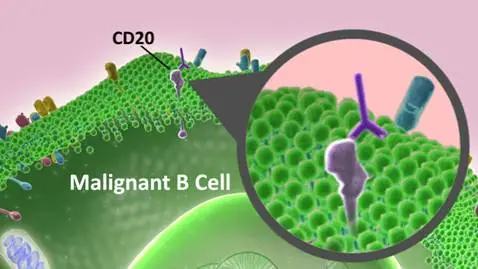
Rituximab was approved for the treatment of non-Hodgkins lymphoma based on its ability to bind the CD-20 antigen on normal and malignant B-cells. Cells marked in this way are then attacked by the natural defenses of the body. Since stem cells don’t have CD-20 the B-cells will regenerate after treatment.
Using chimeric monoclonal antibody drugs was definitely a step in the right direction, exhibiting improved tolerance, however, immunogenicity was still observed from human anti-chimeric antibodies (HACA). Further improvement was seen with humanized monoclonal antibody drugs which contain minimal regions of mouse antibody. Still, in some cases, immunogenicity issues are observed due to human anti-humanized antibodies (HAHA).
I know that HAHA follows the naming convention that was established but to me, this seems an unnecessarily cruel acronym. ‘Thought you could create a monoclonal antibody drug that evades the immune system? HAHA’.
Most recently the use of phage display and transgenic animals have led to fully human monoclonal antibody drugs. These have become the leading source of approved monoclonal antibody drugs.
Although monoclonal antibody drugs have been used as therapies for a variety of ailments the majority of the approvals have been for treating cancers or auto-immune diseases. Multiple lymphoma treatments are counted in the disease targets for monoclonal antibody drugs. As are cancers of the breast, lung, colon, brain, liver, and more.
Not only are diverse cancers targeted by monoclonal antibody drugs but the mechanism of action can also be diverse. We have already seen rituximab’s ability to mark a cell so that it is more easily recognized by the immune system. Other monoclonal antibody drugs block growth factor function by binding to and inhibiting growth factor receptors. For example, pertuzumab and trastuzumab bind to the HER2 receptor and block it from forming a dimer with HER3 or another HER2 protein respectively. In combination, the block HER2 function and therefore can be used as a treatment in certain types of breast cancer.
In addition, the monoclonal antibody can be modified. This is done to achieve targeted delivery of a payload be it a radioisotope, toxin, or another active conjugate. Furthermore, so-called, bi-specific monoclonal antibody drugs bind to both an antigen and an effector cell. Thus enhancing the attraction of the elimination function of the immune system.
One last area, with regard to monoclonal antibody drugs, that is of increasing interest is the fact that many of the original monoclonal antibody drugs are reaching the end of their patent. As such, it is hoped that similar treatments will soon be available. This has led to the increased production of biosimilars that hope to find room alongside the original monoclonal antibody drugs. In order for these replacement therapeutics to receive approval, they must go through a rigorous screening to show at least equal efficacy and safety as the original. Needless to say, this can be an expensive proposition so characterization prior to putting forth a candidate will be an important field going forward.
It is in this arena of characterization that BMG provides many useful tools. Whether you are simply quantifying antibody production or looking at the monoclonal antibody drug antigen interaction, monitoring ligand-receptor interaction, or watching the effect of treatments on cell health outcomes. We have the sensitivity needed for the detection of these important tests in a variety of different applications. Be it fluorescence, luminescence, FRET, BRET, TR-FRET, or fluorescence polarization we can equip you with the ability to detect important outcomes, even in cell-based assays.
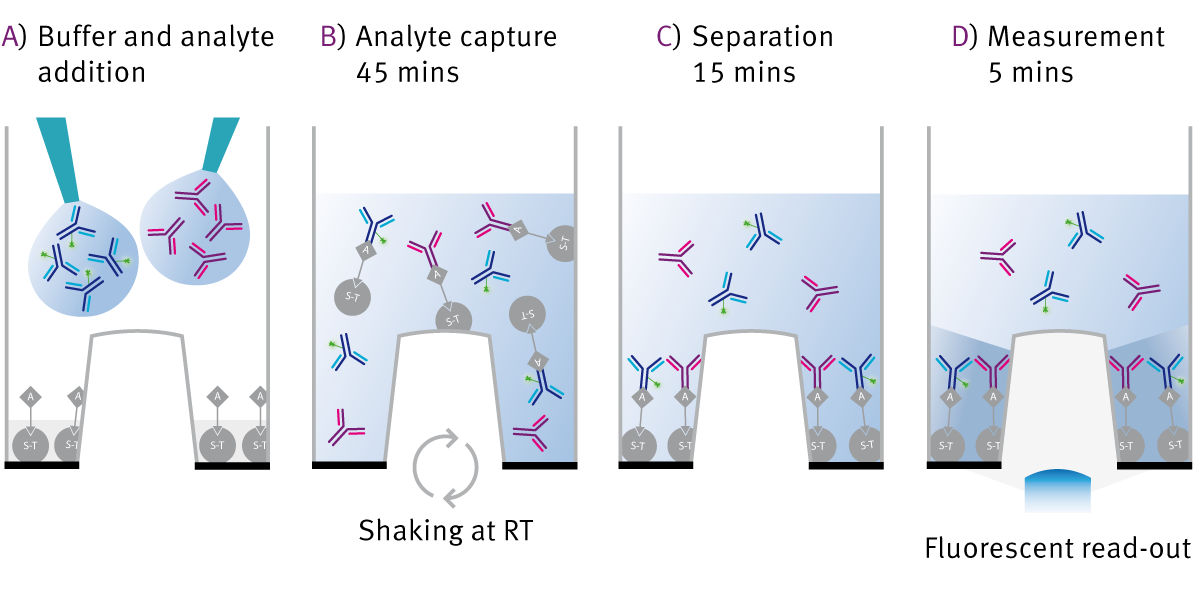
Any of BMG’s plate readers which are capable of detecting fluorescence can be used with plates from PAIA Biotech. We have shown that these plates are useful in quantifying monoclonal antibody production in a relatively high throughput fashion. This makes it possible to use this assay platform to screen for best-producing clones.
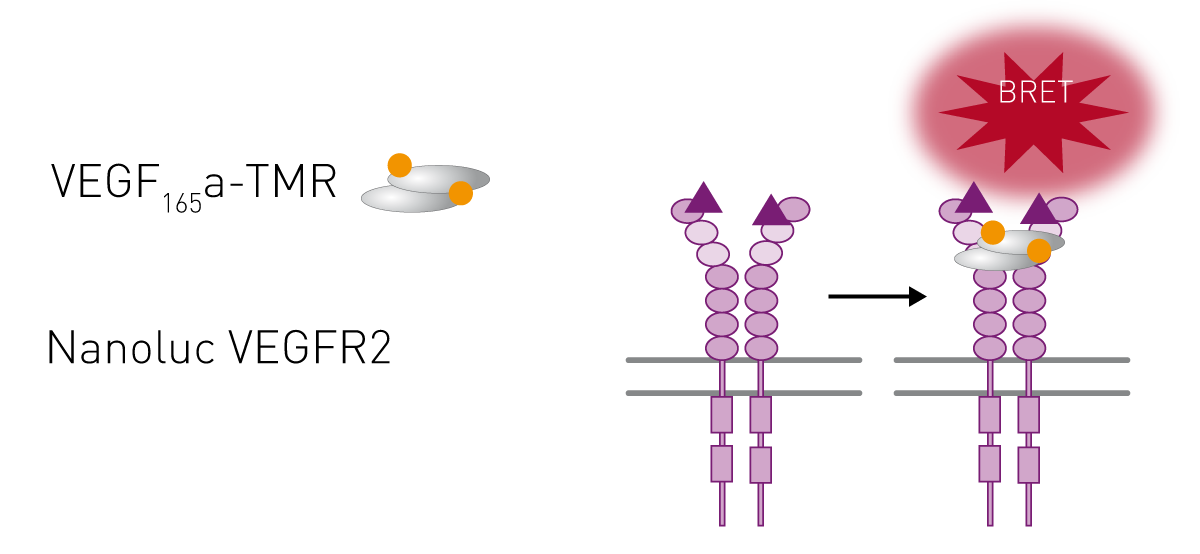
BRET assays are an excellent choice to screen for protein-protein interaction, be it the interaction of antibody with antigen or monitoring alteration in the interaction between a receptor and its ligand. A further advantage is that these assays can be done using a cell-based approach. For example, we have shown the performance of our readers to monitor VEGF interaction with its receptor (fig. 3). A similar approach could be a very useful tool if you are seeking to develop a biosimilar to bevacizumab.
 The use of monoclonal antibody drugs has already led to improvement in therapeutic outcomes for a number of diseases, especially cancers. We at BMG are excited to see what the future holds!
The use of monoclonal antibody drugs has already led to improvement in therapeutic outcomes for a number of diseases, especially cancers. We at BMG are excited to see what the future holds!Absorbance plate reader with cuvette port
Powerful and most sensitive HTS plate reader
Most flexible Plate Reader for Assay Development
Upgradeable single and multi-mode microplate reader series
Flexible microplate reader with simplified workflows
Gene reporter assays are sensitive and specific tools to study the regulation of gene expression. Learn about the different options available, their uses, and the benefits of running these types of assays on microplate readers.
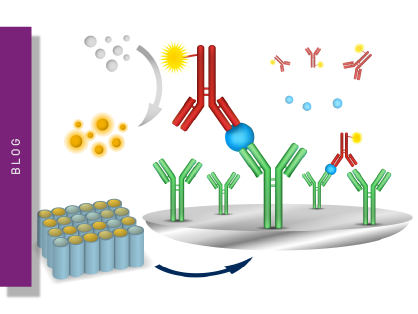
ELISAs are a popular tool to detect or measure biological molecules in the life sciences. Find out how microplate readers can be used to advance research using immunoassays.
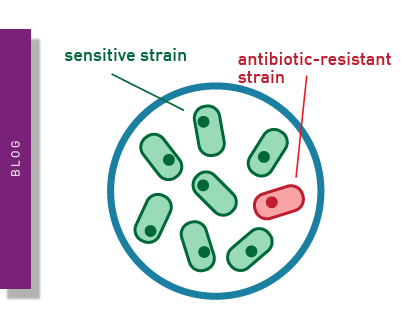
Antimicrobial resistance is a formidable problem across the world. Find out how microplate readers can help tackle resistant microbes.
Next generation sequencing (NGS) technologies for DNA or RNA have made tremendous progress in recent years. Find out how microplate readers can advance the quality control of nucleic acids to facilitate NGS.
Light scattering offers distinct advantages for scientists interested in immunology. Find out how the NEPHELOstar Plus is used for high-throughput immunological tests.
The LAL assay ensures that sterile pharmaceutical products and medical devices are safe for human use. This test can be run efficiently and in high throughput on a plate reader.